A Fresh Look For Fall: The Eyewear Trends You'll Be Seeing Everywhere

What Happens to Your Eyes As You Age A Decade-by-Decade Guide

Are Your Glasses Actually Working As Well as You Think?
Most Popular Posts
Is Joe Biden's Eye Condition a Cause for Concern?

In a recently televised town hall, the live audience raised concern when former vice president Joe Biden's eye began to change colors. As the presidential candidate spoke, the white part of his eye began to turn red. Shortly after the incident media reports exploded, questioning Biden's health and relating the incident to previous health concerns.
The eye condition Biden experienced is called a subconjunctival hemorrhage. In this condition, a very small blood vessel on the outer surface of the eye breaks, allowing blood to pool just beneath the surface. This same process occurs in bruises. However, in an eye, the outer most layer is clear, so the blood appears much brighter than in a bruise, which can be frightening. Isolated occurrences of subconjunctival hemorrhages are not typically indicative of any serious pathology. They can arise from episodes of coughing, sneezing, valsalva, rubbing, and are more common in people who are taking blood thinning medications. Subconjunctival hemorrhages are almost always painless and do not impact vision. There is no treatment, but they will usually resolve fully within a few days to weeks.
Here you can find more information along with a photo of the former vice president during the town hall appearance.
Diabetic Eye Care
It is important for any patients with diabetes (type 1, type 2, or latent autoimmune diabetes) to have annual eye exams as they are at an increased risk of developing many eye conditions and complications. Early detection of any potential problem will lower the risk of vision loss from diabetes. The doctors at Koetting Eye Center are trained using the latest technology to detect and monitor the earliest signs of diabetic eye disease.
In what ways can diabetes affect one’s eyes?
- Blurred vision: When uncontrolled, fluctuations in blood sugar can cause quick changes in glasses or contact lens prescriptions. This is because a higher concentration of sugar inside the natural lens of the eye causes swelling of the lens. It is important that eyeglasses and contact lenses are not prescribed in patients experiencing high fluctuations in blood sugar, as the prescription is likely to change once the blood sugar is controlled.
- Cataracts : It is common for patients with diabetes to develop cataracts at a younger age than average. Symptoms include: blurred or cloudy vision, poor color contrast, glare, and difficulty driving at night.
- Glaucoma: As blood vessels weaken from diabetes, new blood vessels may form in an effort to restore blood flow throughout the eye. In rare cases, these blood vessels will block the area that drains fluid from the eye, resulting in an increase in eye pressure. If left untreated, elevated eye pressure can damage the optic nerve and cause permanent vision loss.
- Diabetic retinopathy
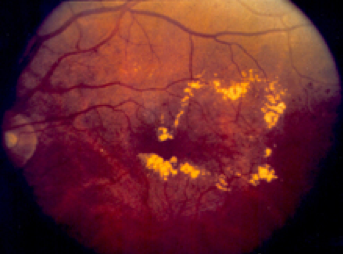
Diabetes is a condition that affects the small blood vessels in the body. Over time, the disease causes the walls of these blood vessels to weaken, eventually allowing fluid and blood to leak outside of the blood vessels. The retina is especially susceptible to this leaking because it has a high concentration of small blood vessels. Damage to the retina from diabetes is termed diabetic retinopathy and is a leading cause of blindness in adults. In most cases, this is completely preventable with close monitoring and tight blood sugar control. Early stages of diabetic retinopathy usually has no symptoms; which makes it so important for patients with diabetes to have annual exams. As diabetic retinopathy progresses, it can be divided into two categories: nonproliferative (NPDR) diabetic retinopathy and proliferative diabetic retinopathy (PDR).
Nonproliferative diabetic retinopathy is the earlier, less severe form of diabetic retinopathy. This occurs when the retinal blood vessel walls begin to break down and allow fluid or blood to leak into the retina. The location of the leaking blood vessels determines if the vision will be impacted. Fluid leaking in an area called the macula is termed diabetic macular edema. Diabetic macular edema is treatable using injectable medication and laser treatment, but the best outcomes come when detected early.
Proliferative diabetic retinopathy occurs when new, abnormal blood vessels grow in the retina. These blood vessels are brittle and cause many problems in the eye, including severe vision loss from leaking vessels and retinal detachments. Depending on the severity, PDR is usually reversible and vision loss is preventable with injectable medication and laser treatment.

Your role in reducing the risk of diabetic eye disease
Blood sugar control is the best way to prevent vision loss from diabetes. Diet, exercise, and medical management by an endocrinologist are the best ways to keep your blood sugar under control. It is imperative to schedule an annual eye exam with a thorough retinal examination. Ocular conditions associated with diabetes have a much better prognosis when detected early. Call us today to schedule your annual diabetic eye exam.
What is Legal Blindness?

Many of us can remember watching the 1992 Olympics in Albertville. Nancy Kerrigan competed as a figure skater, but her mom was not in the stands. She was beneath the stands with Nancy's father watching on a television set. Brenda Kerrigan is legally blind. She lost all of the vision in her left eye and most of the vision in her right eye in 1972 when she contracted a rare virus. Because she could not see anything at a distance, the only way she could watch her daughter skate was to stand very close to the television. At that time, this situation brought a lot of attention to the condition known as Legal Blindness and Nancy would eventually start the Nancy Kerrigan Foundation which raises money for the visually impaired.
But what is Legal Blindness? The term Legal Blindness was defined to help people receive government assistance from the Social Security Administration and to be used by the Department of Motor Vehicles to measure vision and keep our roads safe. To be considered Legally Blind, you must meet at least one of two criteria regarding visual acuity and/or peripheral vision.
Legal Blindness differs from Total Blindness in that a person who is considered Legally Blind will still have some vision whereas a Totally Blind person will not be able to perceive any form or light.
A person who is Legally Blind has a CORRECTED visual acuity of no more than 20/200 in their best seeing eye, or a field of vision that is 20° or less in their best seeing eye.
Let's break that down.
The standard for visual acuity in the United States is measured by the Snellen test. Normal visual acuity is classified as 20/20. In the Snellen test, you are shown a chart that is 20 feet away consisting of letters which get smaller as they progress down the chart. Each line of letters is assigned a number based on what a "normally sighted" person can see at 20 feet. Some people will see the 20/20 line perfectly. Some people will see lines with even smaller print than the 20/20 line clearly. They are the eagle-eyed folks with 20/15 vision or better. Some will not even be able to make out the big E at the top of the chart at 20 feet. The standard for legal blindness is 20/200. This means the person in question sees at 20 feet what a person with normal visual acuity sees at 200 feet. In other words, their vision is ten times worse than that of a normally sighted person.
But wait. In order to be considered Legally Blind, you must have a CORRECTED visual acuity of no more than 20/200. Corrected visual acuity is your vision with corrective lenses- glasses or contact lenses. Most people who are nearsighted or farsighted or have astigmatism are fully correctable to 20/20. This means that once they put on their glasses or contact lenses, they can read the chart every bit as well as a "normally sighted" person. In order to be considered Legally Blind, your vision must be WORSE than 20/200 in your BEST eye while you are wearing your glasses or contacts. So, how poorly you see without your glasses or contact lenses has nothing to do with it. As long as your vision can be corrected to better than 20/200 in one eye with corrective lenses, you are not considered to be Legally Blind no matter how nearsighted, farsighted, or how much astigmatism you have. Also, if your corrected vision in one eye is less than 20/200 but you can see better than 20/200 with glasses or contact lenses in your other eye, you are not considered to be Legally Blind.
The second criteria for determining Legal Blindness has to do with Peripheral or Side Vision. "Normally Sighted" people have a lateral or side field of vision that is 180º. This means that even while you are looking straight ahead, you can see a person standing at your side. Peripheral vision is important to everything we do. We rely on it when walking around, driving a car, or crossing a busy street. Some people have very good eyesight and can see tiny letters from far away, but they cannot see a person standing beside them due to poor peripheral vision. If a Visual Fields test reveals that your field of vision is severely restricted to 20º or less (also known as tunnel vision), you are legally blind; even if you can see 20/20 on an eyechart.
So, what are the causes of Legal Blindness?
There are four leading causes:
Age Related Macular Degeneration (AMD or ARMD)- a leading cause of vision loss in Americans aged 60 or older, AMD occurs when the central portion of the retina known as the macula deteriorates. The macula is responsible for the sharp central vision required for reading or driving.
Cataracts- a clouding of the lens that causes blurred vision. Although usually age related (over half of all Americans will have a cataract by age 80), some cataracts are the result of genetic disorders and others are caused by diabetes or even trauma to the eye.
Diabetic Retinopathy- a disease found in diabetics caused by changes in the blood vessels of the retinal tissue in the back of the eye. This affects an estimated 4 million American adults over the age of 40.
Glaucoma- a condition in which increased pressure within the eye causes damage to the optic nerve thereby decreasing vision. It is estimated that over 2 million Americans have Glaucoma but only half of those are aware they have it.
What are some resources for those who are Legally Blind?
Legal Blindness is considered a disability, and those who are Legally Blind may receive benefits from the Social Security Administration.
Low Vision aids such as magnifiers, telescopes, and digital devices can help those who are Legally Blind to maximize their remaining vision.
Guide dogs are extremely helpful to those who are Legally Blind.
Can Legal Blindness be prevented?
The most important thing you can do to preserve your vision is to have yearly eye exams. Your Optometrist is not only checking your vision, but also monitoring your intraocular pressure, testing your visual fields, visually inspecting your retinas, and monitoring any risk factors you may have from disease, genetics or lifestyle.
Be sure to eat a healthy and varied diet. Get plenty of green leafy vegetables, and good proteins. Fish is also a valuable source of healthy nutrients for your eyes.
Do not smoke. And if you do smoke, quit immediately! Smoking is one of the leading causes of Macular Degeneration and Cataracts.
Always protect your eyes when outdoors. A good pair of sunglasses or Transitions Light Adaptive Lenses will protect your eyes from the harmful UV rays of the sun.
There are over 1 million Legally Blind Americans. Those who are Legally Blind can still have a very enjoyable life filled with hobbies such as reading, cooking, crafting and more, but Legal Blindness is a very real condition that can greatly affect one's quality of life.
So, now that you know the real facts, the next time someone tells you they are "Legally Blind without their glasses", you can help them to understand the truth.
Myopia Control and Kids
There are a growing number of children becoming myopic (nearsighted) every day. In fact, it is estimated that by the year 2020, 50% of the world’s population will be myopic. The Center for Disease Control (CDC) now recognizes this trend as a global epidemic and encourages eye care practitioners to address these changes. Although myopia may seem harmless and correctable with glasses and contact lenses, that is not always the case. Myopic individuals are at higher risk of sight threatening complications such as glaucoma, retinal detachments, macular degeneration and cataracts. The earlier in life children show signs of nearsightedness, the more likely they are to progress and experience these problems.
What Causes Myopia?
The question is often asked, “why are we seeing a shift in more children developing nearsightedness?”. While there might be a genetic link, the answer is not all genetics like once thought. Myopic parents have children with a predisposition to nearsightedness but are not guaranteed this destiny. We know this as we see highly nearsighted parents with children that have varying degrees of myopia. It is believed that myopia development is a product of the environment around us. This has the largest effect on myopic development starting at the early grade school years through late teens. Children are spending more time indoors doing near work than they were 25 years ago. Between digital devices, studying, reading and videogames, children are putting more stress on their visual systems than in the past. Our eyes adapt to this added stress by becoming nearsighted. While the best treatment is to encourage children to spend more time outdoors, running around and getting dirty; more needs to be done as the increasing demand in near work is not going away.

Myopia Control Treatments
There are four main treatments for controlling myopia. The most effective treatment method is chosen based on the child’s current prescription and ability to use contact lenses, eye glasses or eye drops. Treatment is not designed to eliminate future nearsightedness, rather to slow its progression. For example, a child not treated with myopia control might have 8 diopters of myopia by the end of their teenage years. However, that same child treated may only have 4 diopters of myopia by the same time. This may result in a lifetime of fewer nearsighted related complications and eye diseases.
- Orthokeratology (Ortho-K)
This involves using a rigid gas permeable contact lens to gently reshape the front surface of the eye while the child sleeps. The child then enjoys clear vision the next day free of contact lenses or glasses, while getting the full benefit of myopia control. Children as young as 5 are excellent candidates for ortho-k. Studies indicate that this method of myopia control yields, on average, a 50% reduction in myopia progression.
- Atropine Eye Drops
Atropine drops have been used for many years to control myopia progression. They work by limiting the eyes ability to focus up close, which is one of the triggers for myopia progression. Studies suggest that atropine drops reduce myopic progression by upwards of 80%. However, this benefit is limited by the high rebound rate associated with atropine drops. Recent research has found that children using a diluted concentration of atropine drops have a lower likelihood of rebounding.
- Multifocal Spectacles
Children wearing multifocal spectacles compared to single vision spectacles are less nearsighted in adulthood. Like other methods, multifocal eyeglasses work by limiting the amount of stress on the eye during near activities. This treatment results in the lowest reduction in nearsightedness compared to the other three methods.
- Multifocal Soft Contact Lenses
Similar to ortho-k, multifocal soft contact lenses will slow myopia progression by around 50%. While there are many multifocal designs available, studies have found a specific design most effective in slowing myopic progression. The most successful lens design to control myopia is one that features a distance vision corrected zone in the center and a strong reading power outside the center zone.
It Starts with the Parents!
The best and most effective way to take advantage of myopia control is to detect nearsightedness early. Parents should schedule an annual eye examination for their child, even if they do not suspect problems. Children often do not complain of small changes in vision until it is negatively impacting their daily activities. Children undergoing myopia control treatment have less yearly prescription changes and more stable vision. Most importantly, by treating nearsightedness early, children are less likely to encounter future sight-threating vision complications later in life.
Please call today to schedule a consultation to see if myopia control is right for your child!
Privacy
Koetting Eye Center Privacy Policy
This Privacy Policy governs the manner in which Koetting Eye Center collects, uses, maintains and discloses information collected from users (each, a “User”) of the koettingeyecenter.com website (“Site”). This privacy policy applies to the Site and all products and services offered by Koetting Eye Center.
NON-PERSONAL INFORMATION
Non-personal information is statistical data that provides insight into the use of the Site. Koetting Eye Center may collect non-personal information about Users whenever they interact with our Site. Non-personal information may include the type of computing device, the operating system, the browser name, the Internet service providers used, and other similar information.
PERSONAL INFORMATION
Personal information includes name, address, phone number, email address, and other personally identifiable data. Koetting Eye Center may collect personal information from Users in a variety of ways, including, but not limited to, when Users request an appointment or information by completing the request form, subscribe to our mailings, respond to a survey, fill out a form, or register on the site for activities, services or resources that we make available. Users may choose to visit the site anonymously, or may decide to provide name, email address, and other contact information. We only collect voluntarily submitted personal information from Users. Users can always decline to supply personal information with the understanding that it may prevent them from engaging in some activities.
WEB BROWSER COOKIES
Koetting Eye Center may use “cookies” to enhance the User experience. A User’s web browser places cookies on their hard drive for record-keeping purposes and sometimes to track information about them. Users may choose to set their web browser to refuse cookies or to present an alert when cookies are being sent. Some parts of the Site may require cookies to function properly.
HOW KOETTING EYE CENTER USES COLLECTED INFORMATION
Koetting Eye Center may collect and use Users personal information for the following purposes:
– To contact a User who has completed the form to make an appointment or inquire about Koetting Eye Center in order to schedule an appointment and/or provide information to the User.
– To improve customer service. The information you provide helps us respond to your customer service requests and support needs more efficiently.
– To personalize user experience. We may use information in the aggregate to understand how our Users as group access the services and resources provided on our Site.
– To improve our Site. We may use the feedback you provide to improve our products and services.
– To run a promotion, contest, survey, or other Site feature. We may use information you provided to send resources Users agreed to receive about topics we think will be of interest to them.
– To send periodic emails. We may use the email address to respond to inquiries, questions, and/or other requests. If User decides to opt-in to our mailing list, they will receive emails that may include news, updates, related product or service information, etc. The User may unsubscribe from receiving future emails at any time, using the instructions at the bottom of the email.
HOW WE PROTECT YOUR INFORMATION
Koetting Eye Center has adopted standard data collection, storage and processing practices and security measures to protect against unauthorized access, alteration, disclosure or destruction of your personal information, username, password, transaction information and data stored on our Site.
SHARING YOUR PERSONAL INFORMATION
We do not sell, trade or rent User’s personal information. For the purposes outlined above, we may share with our business partners, trusted affiliates and advertisers generic aggregated demographic information regarding our visitors and Users that is not linked to any personal information. We may use third party service providers to help us operate our business and the Site or administer activities on our behalf, such as sending out newsletters or surveys. We may share your information with these third parties for those limited purposes provided that you have given us your permission.
THIRD-PARTY WEBSITES
Users of our Site may encounter links to the sites and services of our partners, suppliers, advertisers, sponsors, licensors and other third parties. We do not control the content or links that appear on these sites and are not responsible for the practices employed by websites linked to or from our Site. These sites or services are constantly changing, and have their own privacy and customer service policies. Browsing and interaction on any other website, including websites that have a link to our Site, is subject to that website’s own terms and policies.
ADVERTISING
Any ads appearing on our Site may be delivered to Users by advertising partners, who may use cookies. These cookies allow the ad server to recognize your computer each time they send you an online advertisement, and to compile non-personal information about you or others who use your computer. This information allows ad networks to deliver targeted advertisements that they believe will be of most interest to you. This privacy policy does not cover the use of cookies by any advertisers.
GOOGLE REMARKETING
Some of the ads may be served by Google. Google’s use of the DART cookie enables it to serve ads to Users based on their visit to our Site and other sites on the Internet. DART uses “non-personally identifiable information” and does NOT track personal information about you, such as your name, email address, physical address, etc. You may opt out of the use of the DART cookie by visiting the Google ad and content network privacy policy at http://www.google.com/privacy_ads.html
CHANGES TO THIS PRIVACY POLICY
Koetting Eye Center may update this privacy policy at any time. When we do, we will adjust the revision date at the bottom of this page. We encourage Users to frequently check this page for any changes and stay informed about how we are helping to protect the personal information we collect. You acknowledge and agree that it is your responsibility to review this privacy policy periodically and become aware of modifications.
YOUR ACCEPTANCE OF THESE TERMS
By using this Site, you signify your acceptance of this policy and terms of service. If you do not agree to this policy, please do not use our Site. Your continued use of the Site following the posting of changes to this policy will be deemed your acceptance of those changes.
RETURN AND REFUND POLICY
Thanks for shopping at Koettingeyecetner.com
If you are not entirely satisfied with your purchase, we're here to help.
Returns
You have 15 calendar days to return an item from the date you received it.
To be eligible for a return, your item must be unused and in the same condition that you received it.
Your item must be in the original packaging.
Your item needs to have a receipt or proof of purchase.
Refunds
Once we receive your item, either by mail-in original packaging or returned to one of our locations, we will inspect it and notify you that we have received your returned
item. We will immediately notify you of the status of your refund after inspecting the item.
If your return is approved, we will initiate a refund to your credit card (or original method of payment).
You will receive the credit within a certain amount of days, depending on your card issuer's policies.
Shipping
You will be responsible for paying for your own shipping costs for returning your item. Shipping costs are nonrefundable.
If you receive a refund, the cost of return shipping will be deducted from your refund.
Contact Us
If you have any questions on how to return your item to us, contact us.
Blue Light Protection
Could an eye exam help you get a good night's sleep?
If you are having trouble sleeping at night, blue light may be the culprit, and glasses or contact lenses could be the solution.
Today's digital technology is better and more convenient than ever. We love our computers, tablets and smart phones. Stuck waiting for an oil change? No problem. Scroll through Instagram or Facebook, play a game, catch up on email or even watch a movie. Our lives are full of modern conveniences that help with many things.
However, digital screens emit harmful blue light, and without proper protection, those conveniences could be costing you a restful night's sleep along with increasing your long-term risk to eye health complications. At Koetting Eye Center, we offer the latest cutting-edge technology in glasses and contact lenses to combat blue light. In fact, our practice was first in the St. Louis area to receive the new Oasys with Transitions soft contact lenses. And for those that wear glasses, we offer many lenses with built-in blue light protection.
Get the Details!
Numerous studies have shown that individuals who are highly engaged in a digital lifestyle are experiencing more eye strain. We also know that too much blue light exposure can increase the aging process of the eye and result in acceleration of age-related eye conditions such as cataracts and macular degeneration. In addition to the blue light emitted from digital screens, the transition from incandescent overhead lighting to LED lighting adds to the bombardment of blue light.
To understand blue light and its effects on the eyes, it is helpful to look at a visible light spectrum of electromagnetic radiation. The spectrum is comprised of different wavelengths of light varying in length from 380-700 nanometers. Shorter wavelengths of light have higher energy and are more likely to cause damage to the eyes. Blue light, also referred to as high energy visible (HEV) light, contains the shortest wavelengths, ranging from 380-500 nanometers. This high-energy blue light is absorbed by the lens of the eye and the retina, which is why these structures are susceptible to damage.
Blue Light and Melatonin
One of the major concerns with blue light that is often over looked is its effect on our sleep cycle. Melatonin is a naturally occurring hormone in the human body that regulates our wake-sleep cycle, or circadian rhythm. Blue light emitted from the sun is important in controlling the levels of melatonin in our body throughout the day. During the day, blue light released from the sun suppress the amount of melatonin produced and keeps us feeling awake and alert. In the evening, when the sun is set, melatonin production increases, making us feel tired and ready for bed. This is when artificial blue light from digital devices and LED lights becomes a problem. Blue light exposure prior to sleep decreases our body’s production of melatonin, resulting in wakefulness and a delayed or disrupted sleep cycle. There are many physical and psychological implications of not getting a full night sleep. It is recommended to minimize blue light exposure a minimum of two hours before bed. Today, most digital devices have a blue filter mode you can program to turn on in the evening, as well as commercially available blue light blocking screens for computers. While these modifications help minimize blue light, they do not eliminate it.
Be Proactive, Not Reactive!
Digital devices and LED lighting are a big part of our lifestyle and will continue to be. In fact, unless you printed this article, you are most likely reading it on a digital screen and being exposed to blue light. The goal is not to eliminate all blue light as some blue light is an important part of our wake-sleep cycle. However, moderation is the key. With the advent of blue blocking glasses and contact lenses, we can now control blue light exposure throughout the day.

If you are experiencing side effects from blue light or are concerned about its long-term effects on your eyes, call today for an appointment. Our doctors can help guide you to the perfect solution to fit your lifestyle and provide you the very best protection from this very real threat.
Macular Degeneration
What is macular degeneration?
Age-related macular degeneration (AMD) is a condition that causes disruption to a small area of the retina called the macula. The macula is about 5 millimeters in size and is responsible for our central vision, allowing us to see fine detail. As the macula begins to degenerate in AMD, patients experience blurred or distorted central vision. AMD is the leading cause of blindness in people over 55 and impacts more than 10 million people in the United States.
A properly functioning retina contains many layers that all work together to process light into clear vision. Beneath these retinal layers is another thin layer responsible for supplying nutrients and removing wastes from the retina, called the retinal pigment epithelium (RPE). In AMD, the RPE loses the ability to rid the retina of waste products, resulting in a buildup of deposits called drusen. It is important to know that, in most cases, patients with a few small drusen never progress to severe AMD and central vision loss. In patients with progressive AMD, drusen increase in size and number. This results in a lack of nutrients supplied to the retina.
Dry vs. Wet Macular Degeneration
As the nutrient supply to the retina weakens with AMD, blood vessels sprouted from the surrounding layers of the eye infiltrate the diseased macula. This is the eye’s attempt to provide nutrients to this undernourished area of retina. Unfortunately, these newly developed blood vessels are very fragile and often leak blood into the macula. If these new blood vessels grow and leak, it is called wet AMD (or exudative AMD). Wet AMD occurs in only 10% of all AMD cases. Vision loss caused by wet AMD often occurs much faster than dry AMD. Most cases of AMD are dry (or non-exudative AMD), meaning these blood vessels never develop. It is important for the doctor to make this distinction because the treatment and management for dry versus wet AMD is much different.
What are the risk factors for AMD?
- Smoking
- Having a family history
- Obesity
- A diet high in saturated fat
- Age over 50
- Caucasian ethnicity
- Excessive exposure to UV light
What are the symptoms of AMD?
- blurred central vision
- distorted or wavy vision
- difficulty reading
- change in color vision
Are there treatments or preventative measures?
Unfortunately, there are no proven curative treatments available for patients with AMD. However, there are measures that can be taken to help combat and slow the progression of the disease. A specific formulation of antioxidants and vitamins, called the AREDS 2 formulation, has proven effective in helping patients with mild AMD. Studies found that taking these vitamins lowers the chances of mild AMD worsening to more advanced forms. For smokers, cessation is another important step to lower the risk of progression. In addition, sunglasses should be worn outside to protect the retina from excessive exposure to ultraviolet light.
For wet AMD, development and growth of new blood vessels can be managed with laser treatments, photodynamic therapy, and/or anti-VEGF injections. These treatments are very effective at halting further progression and sometimes result in improved vision.
Is there anything that can help me see better?
While there are currently no treatments to permanently reverse the vision loss caused by AMD, we do have access to rehabilitation services and low-vision devices that help optimize patients’ functional vision. These specialty devices include hand-held and video magnifiers, computer programs, large print books, and other ophthalmic devices.
SIX POPULAR EYECARE MYTHS DISPELLED

Most (or all) of us have heard these statements at least once in our lives: "Don't cross your eyes or they'll get stuck like that" or "Don't sit too close to the TV or you'll ruin your eyesight!" Are these just things moms say to get kids to behave? What are the actual facts? Do you think you can spot the truth from the fiction? Test yourself below:
1.) Eating lots of carrots will improve your vision.
False.
Carrots are delicious and healthy. They are packed with vitamin A which is important for your eyesight and they are always a good choice for your diet. However, lots of foods contain vitamin A including eggs, broccoli, spinach, sweet potatoes and oranges. As long as you are making healthy food choices and getting plenty of fruits and vegetables, your normal diet should provide plenty of this vitamin. Carrots are good for you but no matter how many you eat it will not improve your vision.
2.) If you cross your eyes they will stay that way.
False.
The legend goes that if you cross your eyes they will stay that way- especially if someone slaps you on the back at the same time! The truth is that although the muscles in your eyes will get tired if you cross them for an extended period of time, there is no medical evidence to suggest that they will get stuck like that. Eyes are meant to move in all directions and no amount of crossing them will make it permanent. In face our eyes naturally converge or come together when we are reading or looking at things up close so when you purposefully cross your eyes you are just exaggerating this natural response. However, if you notice that your child is crossing one eye constantly, schedule an evaluation by an eyecare professional.
3.) If parents have poor eyesight, their children will inherit the trait as well.
Sadly, this one is sometimes true.
The two most common and serious types of eye disease among adults, Macular Degeneration and Glaucoma are inherited in most cases. Researchers have found a strong family connection in a large percentage of patients with Macular Degeneration (a condition where the central part of the retina begins to deteriorate causing loss of vision), and they are working to identify the specific genes involved.
There are also genetic links for conditions such as Strabismus and a condition called Retinitis Pigmentosa (which causes night blindness and gradual loss of vision).
But what about more common refractive errors such as nearsightedness (myopia), farsightedness (hyperopia) and astigmatism? Research shows these conditions are often caused by inherited genetic markers. In fact, people with a genetic predisposition toward refractive errors such as myopia, hyperopia and astigmatism are ten times more likely to develop them. Heredity is tied to 50% of cases of astigmatism, and to 50% of cases of color blindness as well. And, parental nearsightedness significantly increases a child's chance of becoming nearsighted. A child who does not have a nearsighted (myopic) parent has only a 2.5% chance of becoming nearsighted, but when one parent is nearsighted, the child's odds of becoming nearsighted increase to 20%. And if both parents are nearsighted, that child's chances of developing myopia increase to 33%. In other words, one in three children whose parents are both myopic will become myopic.
However, the blame is not entirely genetic. There are many environmental factors which affect our eye health and vision that can be controlled. For instance, wearing UV protective sunwear while outdoors, and maintaining a diet rich in green leafy vegetables, fish and fruit will help to prevent age related eye disorders. Also, because smokers have four times the risk of developing cataracts, age related macular degeneration and cancer, do not smoke! And if you do smoke, quit as soon as possible! Lastly, be sure to give an accurate and complete family history to your eyecare professional so they can be sure to monitor any increased risks you may have.
4.) Wearing glasses will make your eyes dependent on them and make your eyes weaker.
False.
Wearing glasses will not make your eyes worse. Some eye conditions such as nearsightedness or farsightedness will worsen over time, but that has nothing to do with glasses. This belief that glasses make your eyes weaker is acutally based on the perception you will get once you see your corrected vision compared to your uncorrected vision. For instance, if you don't wear glasses or if the prescription in your glasses is not strong enough due to a change in your vision, you may not necessarily perceive how badly you are seeing because you don't have anything to compare it to . Once you begin wearing your new prescription lenses, you will realize how much better the world looks with them on!
5.) Sitting too close to the television will ruin your eyesight.
Sorry mom, this is false.
It's common for kids to sit close to the TV, but the reason is simply to become more engaged in it, not really to see it better. It's really about the immersion in the sights and sounds and story. There is no truth to the myth that sitting too close to the television will make your eyes weaker.
However, if your child cannot comfortably see the television from the couch, it is time to visit your eyecare professional.
6.) You only need an eye exam if you notice a problem.
False.
You may think your eyesight is fine or think you don't need to worry about eye problems until you reach your forties, but this doesn't mean you should skip your yearly eye exam. A comprehensive eye exam is about much more than monitoring your glasses or contact lens prescription. Your eye doctor will also check for diseases such as glaucoma which can show up long before you reach old age. Additionally, your eye doctor may notice signs of other diseases such as diabetes or high cholesterol. Regular eye exams are an important part of your overall health. And, yearly eye exams will give you the best chance at early detection for some of the most devastating eye conditions which may end up saving your eyesight!
Why do we need your Photo ID?

Medical forms are an important part of your medical records. They help us understand your health concerns, family health history, manage billing, and protect your privacy. We ask you to fill out forms each year so we can keep this information up to date and provide you with the best possible care. We will also ask you for updated insurance cards and photo I.D. each time you come.
One of the ways we provide you with the best possible eyecare is through the use of electronic medical records.
Along with the use of electronic medical records comes great responsibility on our part. We recognize this fact and are dedicated to keeping your information safe through multiple firewalls, and safeguards. We also conform to the strict guidelines put forth by HIPAA (Health Information Privacy Act) and CMS (Center for Medicare Services) “meaningful use” requirements. By achieving these “meaningful use" requirements, we improve healthcare quality and patient outcomes.
In short, it is not our goal to invade your privacy or put your Personal Health Information at risk, but rather we are doing our best to follow the rules, meet all requirements, and provide the best possible care for our patients.
CMS has the strictest requirements of any health insurance, so by utilizing those standards across the board- even for private insurance and private pay patients- we are confident that we are making the very best effort to provide our patients superior service while safeguarding both your personal information and patient rights.
We include your photo ID in your patient record for a couple of reasons.
Firstly, for your safety. When we can verify your identity by looking at your photo, it eliminates the risk of treating the wrong patient. You might be surprised at how many patients will respond to the incorrect name. We want to be sure we have the proper chart pulled up when we are treating you.
Secondly, it helps to prevent Insurance Fraud. We do not suspect that you are committing fraud, however, it is a very prevalent problem and Medicare requires us to keep a photo ID on file for each patient to verify that they are the insurance holder. In fact, many insurance companies require this and if we are audited by an insurance company and they do not see a photo ID in your chart, we can incur fines or other penalties.
We want you to enjoy your visit at Koetting Eye Center, we want to make things as easy and pleasant as possible, but we do also have to follow these requirements.
Rest assured that we take your privacy and your information seriously and we are dedicated to protecting you and to providing the very best service possible.
Advancements in Dry Eye Therapy
Over the last several years, researchers have learned significantly more about dry eyes. Gone are the days where we are restricted to artifical tear drops to sooth symptoms of dryness. What we know is that the old name "dry eye syndrome" is a vague explanation of symptoms for a more rooted problem. The new approach is to first identify the source and individualize a treatment based on that.
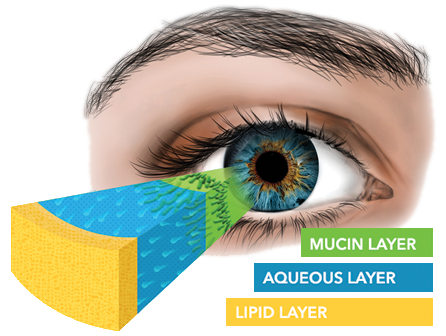
Our tear film is made up of three main components which interact like layers of an onion: mucin, water, and oil. The inner most layer is made of mucin, which adheres the tears to the eye like puddy. Just outside of that is the aqueous, or water, component that lubricates the surface of the eye. Lastly, and arguably the most important component, is oil. Oil, or lipids, act like the shield that sits on the outer most layer of the tearfilm. For better visualization think about oil floating on top of a body of water. This oil provides a nice smooth surface for clear vision and protects the underlying aqueous layer from air. Without a structurally sound lipid layer the water layer will quickly evaporate, directly exposing the eye to wind and irritating air particles.
What we have learned is that this vital oil is actually produced from glands within the eyelids, called meibomian glands. These are modified versions of the same glands that produce oil on your skin. These meibomian glands are prone to clogging and obstruction. When these glands are not producing oil as they are intended to it is called Meibomian Gland Dysfuntion (MGD). MGD is the leading cause of dry eyes and is found in about 85% of patients with dry eye symptoms. MGD is a chronic, progressive condition that without intervention may continue to worsen until the glands become completely unfunctional.
Once lost, these glands are very difficult to revive. We use heat therapy in the form of warm compresses to melt the stagnant oil so that it may flow more freely. Additionally, we emphasize the importance of complete blinks which promote the release of oils from the glands onto the surface of the eye. For symptomatic relief artificial tears containing lipids are recommended as needed; although, it is important to know these will not help to improve gland function. Omega-3 fatty acid supplements have been shown to reduce ocular surface inflammation which drives this chronic condition. Antibacterial lid wipes and hypochlorus acid sprays work to eliminated any over population of unwanted microbes on the eyelids and clean the gland surfaces. While these therapys help the glands function and may provide short-term relief of symptoms, they do not clear deep obstructions which leave the glands unfunctional.
A new treatment, called the Lipiflow system, uses heat and pressure to clear blocked meibomian glands by applying heat directly to the glands on the inner eyelid surface. Heat rapidly and efficiently raises gland contents, liquifying any blockages making it easier to remove from the gland. Gentle pressure is applied to the outside of the lid from the base of the gland to the gland opening removing blockages and flushing dead cells from the gland. During this process stagnant gland tissue may be removed from the glands. Maintaining normal meibomian gland health and function is critical to the long-term maintenance of ocular surface health and good vision. The Lipiflow treatment is an in office procedure lasting about 12 minutes per eye. This deep cleaning is repeated in most cases every one to three years. We are pleased to offer this treatment option at Koetting Eye Center. Please ask one of our doctors how the Lipiflow system can help you.
Click here for a link to recent news story about the benefits of the Lipiflow.